

Australia’s Excess Deaths Inquiry Suppresses Majority of Submissions, Omitting Key Evidence from Record

By Rebekah Barnett: Dystopian Down Under
Two thirds of submissions made to the Australian Government’s Excess Mortality Inquiry have been suppressed and key evidence omitted from its concluding report, calling the inquiry’s integrity and findings into question.
The world-first inquiry set out to investigate why record-high numbers of Australians have died in recent years, including non-Covid deaths, at levels not seen since World War II.
On Friday, the Excess Mortality Inquiry committee handed down its report, concluding that Covid is the “key driver” of Australian excess mortality, both “directly and indirectly”.
However, it has come to light that the committee buried the majority of submissions made to the inquiry, acknowledging only 59 (31.5%) of 187 submissions received on the public inquiry page.
A review of several withheld submissions and evidence submitted during the inquiry’s public hearing reveals that key evidence raised in the inquiry process has been entirely omitted from the committee’s report.
The committee’s suppression of this evidence raises the question: Did the committee follow the evidence, or did it discard the evidence that didn’t follow its preferred narrative?
“Incredibly high” excess mortality
The federal Excess Mortality Inquiry was established in March of this year to identify drivers of Australia’s excess mortality from 2021-2023, and to make recommendations on how to address preventable drivers of excess mortality going forward.
Like many other Western countries throughout the pandemic years, Australia saw “incredibly high” excess mortality that could not be entirely explained by Covid, leading to calls for further Government investigation.
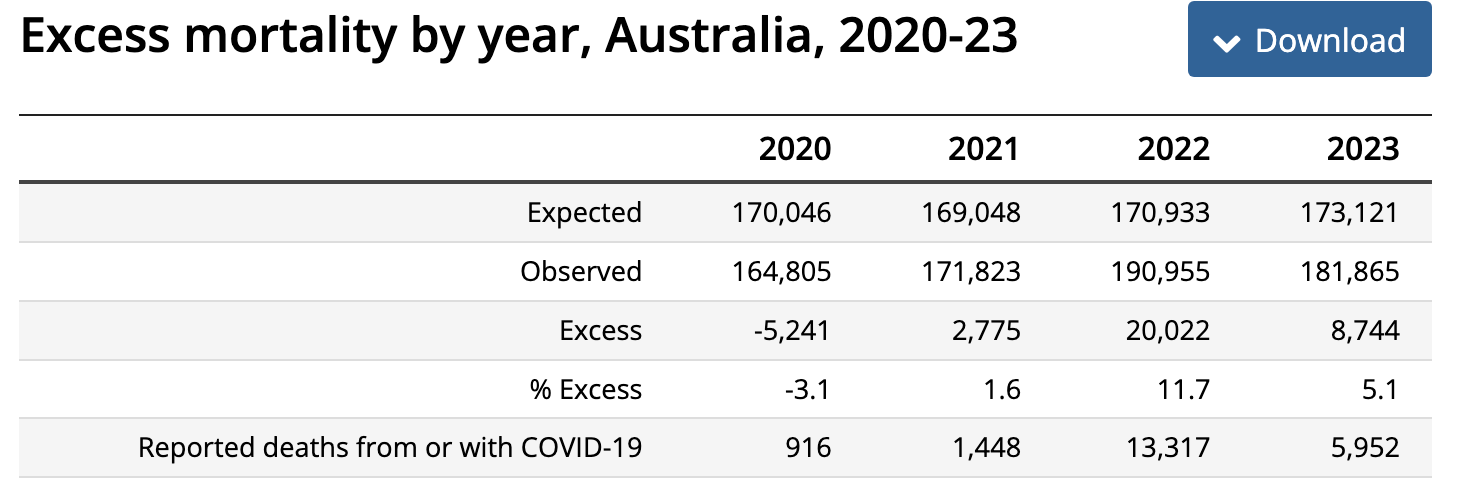
According to analysis by Australia’s peak actuarial body, the Actuaries Institute, excess deaths peaked in 2022 at 12%, an extra 20,200 deaths above the expected baseline. Excess mortality remained high throughout 2023 at 5%, an extra 8,400 deaths. Australian Bureau of Statisics (ABS) figures differ slightly.
Former Actuaries Insitute spokesperson Karen Cutter told news.com.au that “mortality doesn’t normally vary by more than 1 to 2%”, so the excess mortality seen by Australia during the pandemic years is “way higher than normal levels”.
Committee finds: Covid did it
On Friday, the committee released its report outlining key drivers of Australia’s excess mortality. You will probably not be shocked to read the committee’s main finding:
The evidence presented to the committee overwhelmingly pointed to COVID-19 as the key contributing factor to excess mortality during 2021-2023. This included deaths both directly and indirectly caused by the virus.
In arriving at this conclusion, the committee relied mostly on submissions from the ABS, the Australian Institute of Health and Welfare (AIHW), several other Government departments and the Actuaries Institute, which estimated that “total deaths from COVID-19 of 17,200 make up almost two-thirds of the total estimated excess mortality of 27,200” (emphasis mine).
Ironically, the actuaries note that the majority of these deaths occurred after the “vast majority of the population was vaccinated”.
The committee reported that Covid was probably indirectly driving a significant remainder of unexplained excess deaths as well, as Covid can contribute to other leading causes of death in Australia which spiked throughout 2021-2023, including cardiovascular disease, strokes, diabetes and dementia. While cancer is a leading cause of death in Australia, cancer deaths did not significantly increase during this time.
The committee acknowledged that reduced access to healthcare due to the pandemic response may have contributed to the increases seen in the above-mentioned chronic diseases.
The committee also attributed some of Australia’s excess deaths to mortality displacement, noting that Australia experienced lower than expected mortality in 2020 due to reduced circulation of respiratory diseases, delaying some expected deaths into the following years.
Suicide and mental health were discussed, but the committee referred to submissions and testimony suggesting that suicide did not have a statistical impact on excess mortality.
Definitely not the vaccines
Despite receiving “large amounts of correspondence… in relation to vaccine injuries”, the committee dedicated only a single page of its report to discussion of the potential impact of Covid vaccinations on Australia’s excess mortality.
The report quoted just a single submission, from Covid vaccine injury research and advocacy group, COVERSE:
While our organisation does not have statistical evidence that the COVID-19 vaccines have definitely contributed to excess mortality during 2021-2023, we do have evidence of widespread and significant downplaying of vaccine-caused harms, which has concerning implications for current understanding of drivers of excess mortality in Australia.
Having read several submissions to the inquiry which contain information on the inadequacies of Australia’s official record keeping, peer-reviewed data on Covid vaccine harms and evidence of deceptive conduct in the Covid vaccine trials, it is noteworthy that the committee made the editorial choice to feature only the above quote.
Another quote from COVERSE Director Rado Faletič that the committee did not include, but that was highlighted in Senator Ralph Babet’s dissenting report, gives insight into the potential scope of Covid vaccine injury in Australia:
We know, for example, that when the Australian Government’s Vaccine Claims Scheme was launched there were 10,000 people who signed up to receive information. That’s 10,000 Australians who had an adverse reaction serious enough to think they needed compensation. From our perspective and from all of the other bits of information that we’ve collected, we think that’s a lower bound. The true number of people in this country could be 10 times as many as that.
How many of these 10,000 Australians are still alive today, we do not know, because no one is tracking their progress.
The committee rejected the concerns raised by COVERSE and others about the impact of Covid vaccinations on excess mortality because:
Official data show that the vaccines have only killed 16 Australians.
The Actuaries Institute said that in fact, “COVID-19 vaccines have significantly reduced excess mortality” [emphasis in original].
The first claim is a revelation because until now, the media has been parroting the Therapeutic Goods Administration’s (TGA) figure of ‘only’ 14 deaths related to the vaccines. Even still, the number cited by the committee misrepresents the figures supplied to the Inquiry by the ABS. More on that in a soon-to-be-published post.
For the second claim, the Actuaries Insitute cited a single modelling study of New South Wales (NSW) data, from which the actuaries extrapolated to estimate that the Covid vaccines saved more than 50,000 lives nationally.
The study contains too many flaws to list in full. The main ones, however, are the miscategorisation of anyone within 21 days of their first dose of Covid vaccination as ‘no effective dose’; overestimation of the virus mortality risk; and failure to control for age and comorbidities, the primary determinants of Covid severity.
The committee dismissed the entirety of the submissions presenting medical, statistical and anecdotal evidence of Covid vaccine harm within the Australian population on this basis. That’s it. That’s the end of the vaccination section.
Incidentally, the committee dedicated three pages of its report to chastising Senator Babet (United Australia Party) for a single incident of inappropriately editing and disseminating a video of witness testimony from the public hearing, which apparently caused the witnesses some distress. The committee also dedicated one of its five concluding recommendations to further addressing this matter.
The disparity in attention paid to each of these issues gives a sense of where the committee’s priorities lie.
Majority of submissions buried
Two thirds of submissions made to the inquiry were reclassified by the committee as “unpublished correspondence”, effectively hiding them from public view.
In its report and on the inquiry page, the committee acknowledged only 59 submissions. However, Senator Babet’s dissenting report references a total of 187 submissions made to the Inquiry of which 130 had permission for publication.
Only 51 were published by the committee, while 79 (61%) were withheld.
I know that some of these unpublished submissions were withheld despite formal requests from the authors that their submission be made public – myself included.
Committee Chair, Senator Penny Allman-Payne (Greens) did not respond to several emails and a phone message left at her office requesting an explanation as to why the committee saw fit to withhold so many submissions.
Key evidence from unpublished submissions omitted from report
Below, a selection of the evidence submitted to the inquiry that remains unpublished, and that was not mentioned in the committee’s report.
Augusto Roux, Lawyer, Argentina
Roux’s submission presented “evidence that information about serious harms (including deaths) during Pfizer/BioNTech’s phase 3 clinical trial were [sic] deliberately withheld from government drug regulators”.
As a participant in Pfizer/BioNTech’s phase 3 clinical trial, Roux suffered “loss of consciousness, fainting, tachycardia that almost left me near death, and extremely dark urine” after his second dose of vaccination. He was rushed to hospital and was diagnosed with pericarditis with pericardial effusion and liver damage.
Roux alleges that Pfizer first tried to blame his condition on a Covid infection (which he didn’t have). Then, the Principal Ion the trial falsified records, claiming that Roux’s symptoms were caused by a mental health illness (which he didn’t and doesn’t have), alleges Roux. Roux also highlighted irregularities in the recording of deaths within the clinical trial.
Raphael Lataster, Researcher, Australia
Lataster, a former pharmacist and hospital administrator, summarised the peer-reviewed evidence, some of which he authored himself, questioning Covid vaccine safety and effectiveness and pointing to negative effectiveness.
Lataster claims that not only are the safety and effectiveness of Covid vaccines exaggerated in clinical trials and observational studies, but “There is also increasing evidence of negative effectiveness – where the vaccine appears to increase the chance of COVID-19 infection, hospitalisation, and even death”.
Lataster’s research highlights the skewed benefit-risk profile of Covid vaccination for young people. “Hundreds of thousands of young and healthy people need to be vaccinated to prevent a serious COVID-19 hospitalisation,” he said, while recent research indicates “the rate of serious adverse effects in the vaccinated is as high as 1 in 400”.
In a recently published study, Lataster found “clear, statistically significant, correlations between both COVID-19 vaccination rate and total COVID-19 vaccine doses in approximately 30 European countries with excess mortality, persisting into 2024”.
Dr. Melissan McCann, General Practitioner, Australia
Despite being personally invited to make a submission to the inquiry, Dr. McCann’s submission was reclassified by the committee as “unpublished correspondence” without explanation.
Dr. McCann submitted that Vaccine Associated Enhanced Disease (VAED) may be a key driver of Australian excess deaths. Per the World Health Organisation’s (WHO) Brighton Collaboration, VAED is described as a syndrome of “disease enhancement” associated with some viral vaccines, “where those immunised suffered increased severity or death when they later encountered the virus or were found to have an increased frequency of infection”.
This is particularly relevant to Australia said Dr. McCann, where “the overwhelming majority of the population contracted COVID-19, sometimes multiple times, despite being vaccinated”.
The TGA and the Brighton Collaboration both identified VAED as an important potential risk of Covid vaccination, with the latter recommending that all cases of vaccine failure (also called ‘breakthrough infections’) be carefully investigated by authorities.
Additionally, Dr. McCann said that TGA records show that 28% of deaths reported to the DAEN in association with Covid vaccines occurred within one week of vaccination, and the majority occurred within six weeks or less from vaccination, “which is highly suggestive of likely causality based on the temporal relationship”.
The Australian Medical Professionals Society (AMPS)
The committee refused to publish the AMPS submission in full, despite AMPS jumping through hoops to reformat it to the committee’s satisfaction. Only a summary document was published to the log, hyperlinking to the full submission on the AMPS website.
The comprehensive, multi-disciplinary submission contends:
Covid deaths account for 29% of excess mortality at most. While the actuaries and the ABS attributed all Covid deaths to excess mortality, only half of Australian Covid deaths could be considered “excess”, even considering the unusually broad WHO coding for Covid death attribution. (Chapter 4)
Top three causes of non-Covid excess deaths in peak year of 2022:
Deaths with abnormal symptoms and signs where the cause can’t be classified: 2,557 excess deaths (190% increase compared to five pre-pandemic years 2015-2019)
Diseases of the nervous system: 2,066 excess deaths (28% increase)
Diseases of the digestive system: 1,687 excess deaths (28% increase) (Chapter 4)
Excess deaths may be 25% higher than estimated by the ABS. Alternative modelling of Australian cumulative excess deaths throughout 2021-2023 estimates approximately 40,000, as opposed to the ABS estimate of 29,601. (Chapters 5 and 6)
Public health failures are a key driver of excess mortality. Public health policies that were harmful to health include: prolonged lockdowns, vaccine mandates, failure to address key determinants of Covid outcomes such as obesity, failure to promote proven early treatments and misinformation about ivermectin. (Chapters 1 and 2)
Unprecedented rates of adverse event reporting associated with Covid vaccines. Detailed analysis of the TGA’s DAEN and the AusVaxSafety Programme shows that, relative to the number of doses administered, Covid vaccines are associated with unprecedented rates of adverse event reporting, including 400 new types of adverse events not previously reported over the 52-year history of the DAEN. A temporal relationship between excess deaths and the Covid vaccine rollout is observed.(Chapter 6)
The effect of mortality displacement on excess deaths is estimated to be minimal. Mortality displacement likely accounts for no more than one tenth of excess mortality in 2022 onwards. (Chapter 5)
Data gaps prevent rigorous analysis of the impact of vaccination on excess mortality. Linked all-cause mortality data stratified by age and vaccination status are required to make a proper assessment of the effectiveness of the Covid vaccine rollout in the Australian population. To date, no government department has released the linked data or produced its own analysis of all cause mortality by vaccination status. (Chapter 5)
Additional evidence within the AMPS submission includes:
Evidence of an uptick in all-cause mortality with the introduction of Covid vaccines to a zero Covid community. (Chapter 5)
Evidence that Covid vaccine injuries and deaths are under-reported in official record keeping. (Chapters 3 and 6)
Evidence that deaths in the vaccine arm of the Pfizer trial were concealed from government regulators prior to the U.S. Emergency Use Approval (EUA) data cut-off date. (Chapter 7)
Evidence of a 3.7-fold increase in cardiac events in vaccinated vs. placebo arm subjects in the Pfizer trial. (Chapter 7)
Excess Mortality Inquiry Recommendations
At the conclusion of the Excess Mortality Inquiry, the committee made five recommendations to the Australian Government, abridged as follows:
The ABS should address excess mortality data gaps relating to Aboriginal and Torres Strait Islander people, people with disability, and people in rural and regional areas.
The Australian Government should consider the design and compensation arrangements of a no-fault compensation scheme for Commonwealth-funded vaccines in response to a future pandemic event.
The Australian Government should establish the Australian Centre for Disease Control as soon as practicable.
The Department of Health should review and improve its public health information communication strategies.
The Senate should take note that witness participation in public hearings is critical to the committee inquiry process; witnesses should be treated with respect; and Senators should be reminded of the Resolution on the Broadcasting of Senate and Committee Proceedings.
It is unclear that these recommendations will make much of a difference to preventable drivers of Australia’s excess mortality, although it cannot hurt to improve data production and publication per Recommendation 1.
If the Australian CDC is comparable to the American CDC, one could reasonably argue that Recommendation 3 will have the effect of degrading Australia’s ability to respond well to future pandemics, and will likely undermine Recommendation 4.
Recommendation 5 appears to be a direct dig over an unforced error by Senator Babet, which comes across as petty given the subject matter of the inquiry.
Recommendation 2 is welcome. Where governments indemnify vaccine manufacturers, and especially where vaccines are mandated, it is essential that citizens injured by the vaccines be compensated swiftly and adequately.
The federal Covid vaccine injury claims scheme is due to end on September 30th 2024, even though Covid vaccines will still be administered for the foreseeable future. This will leave injured Australians without a safety net.
COVERSE is running a campaign encouraging Australians to contact their federal Member of Parliament to alert them to the fact that the compensation scheme is ending, and to request their support for its extension. Resources are available on the COVERSE website.
A report the committee wanted to write?
During Covid times, the pattern of these government-led inquiries has been to formally rebrand what was at the time a radical departure from scientific and policy consensus as the ‘future pandemic roadmap’ – the new normal.
In this respect, the Excess Mortality Inquiry has been no different. The record will show, effectively:
Covid was such a great threat that it caused record-high excess deaths. The extreme measures taken by our governments saved tens of thousands of lives, with negligible concomitant harms. We shall improve by further centralising our efforts and continuing to strive for equity.
The committee says that the “unpublished correspondence” that it buried “helped the committee progress its understanding of the issues it considered as part of this inquiry”.
However, in suppressing these submissions, the Excess Mortality Inquiry committee appears to have written the report it wanted to write, leaving aside any evidence that might interfere with its predetermined narrative.
A Royal Commission is probably the only option for achieving the level of inquiry and accountability that the Australian public is owed on the Covid era.
Queries regarding the 79 unpublished submissions can be directed to the committee Chair and Members, listed here.
This article was originally published on Dystopian Down Under, Rebekah Barnett’s Substack newsletter. You can subscribe here.
West Australian Rebekah Barnett is one of the most talented young journalists to have come to prominence during the Covid era.
To support her work, share, subscribe, and/or make a one-off contribution to DDU via my Kofi account. Thanks!
Follow Rebekah Barnett on Instagram
Follow Rebekah Barnett’s Substack page

